Selner's Rhinolaryngoscopy Online

John C. Selner, MD
William K. Dolen, MD
Bryan Spofford, MD
Jerald W. Koepke, MD
Endoscopic Images and Annotations - 2. The Nasopharynx
Endoscopic Images and Annotations - 1. The Nasal Cavity
Endoscopic Images and Annotations - 3. The Oropharynx
Endoscopic Images and Annotations - 4. The Larynx
Nasopharynx
 |
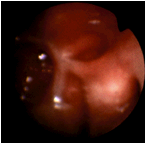
In this view of a normal right posterior nasal passage, the adenoidal pad is seen posteriorly. The eustachian tube orifice, surrounded by the torus tubarius, is on the left at 9 o'clock. Rosenmüller's fossa is the potential space between the posterior torus and the adenoidal pad. |
 |
Another normal view of the posterior right nasal passage with the arch of the posterior choana visualized superiorly. It meets the vomer of the septum at 3 o'clock and appears contiguous with the torus at 9 o'clock. The dimple at 9 o'clock is the eustachian tube orifice, surrounded by the torus tubarius . The adenoidal pad can be seen in the posterior pharynx. The cleft between the torus and the adenoidal pad is Rosenmüller's fossa. (Selner slide #13) |
 |
The rhinoscope is on the floor of the right posterior nasal passage, showing the right posterior nasopharynx in the distance. The soft tissue located at the bottom of this slide is the elevated soft palate in phonation as the patient is saying "K-K-K" or "eeee". This eustachian tube orifice appears patulous or overly patent. Behind the posterior lip of the torus, the adenoid tissue is poorly illuminated and one can not clearly visualize Rosenmüller's fossa. (Selner slide #15) |
 |
This choanal nasal polyp of posterior ethmoid origin was discovered on examination during a weekend course for local physicians. The doctor complained of nocturnal awakenings associated with nasal obstruction. Workup revealed EKG evidence compatible with significant airway obstruction. Removal of this obstruction necessitated dissection of the polyp into 3 segments. |
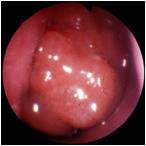 |
Another view of the nasal polyp. |
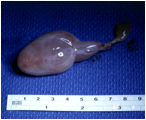 |
A large nasal polyp as removed intact at surgery. |
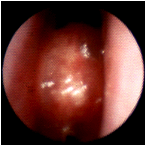 |
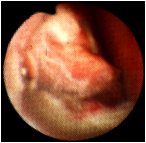
A polyp in the right nasal passage, selected to demonstrate squamous metaplasia, a consequence of dry air inducing keratinization of the mucosa covering the polyp. Normally, polyps are translucent; this mucosa is more opacified. The septum is located at 3 o'clock, the inferior turbinate at 9 o'clock. (Selner slide #28) |
 |
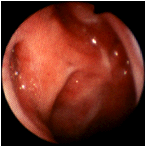
Partial obstruction of the right nasal cavity by adenoidal hyperplasia. The small aperture inferiorly may disappear when the child is sleeping and the palate moves superiorly. This can result in snoring with apnea and mouth breathing with maxillofacial and dental growth abnormalities. |
 |
Partial obstruction of the left nasal cavity by adenoidal hyperplasia. |
 |
Nearly total obstruction of the right nasal cavity by adenoidal hyperplasia. |
 |
The left posterior nasal cavity of a child with disturbed sleep and behavioral manifestations which led to psychiatric intervention. There was an adenoidal facies, disturbed maxillary growth, and the patient was undergoing orthodontic corrective measures, including the use of a palate expander. The septum is located at 9 o'clock. At 11 o'clock is the posterior margin of the middle turbinate, and there is extreme adenoidal hypertrophy, herniating anteriorly through the posterior choana, resulting in complete obstruction. Symptoms were relieved by adenoidectomy. (Selner slide #36) |
 |
The nasopharynx. A prior adenoidectomy has resulted in formation of scar tissue from the posterior torus to the adenoidal pad. |
 |
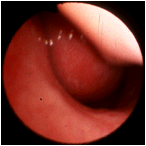
Postadenoidectomy scarring, an incidental finding with fibrous scar tissue bridging from the adenoids across Rosenmuller's fossa to the torus of the eustachian tube located at 8 o'clock. The stellate scar on the right is typical of the postadenoidectomy healing process. (Selner slide #35) |
 |
The left nasal passage. The inferior turbinate is at 2 o ' clock, and the septum is on the left. The smooth vascular structure obstructing the choana proved to be an angiofibroma with origin in the sphenoid sinus. Although this patient was an adult, angiofibromas usually present in adolescent males with a history of nasal obstruction and recurrent epistaxis. It is distinguishable from adenoid tissue by its smoothness and red color; it may also be pulsatile. Angiofibromas may be visualized by angiography or a CT study with contrast. (Selner slide #37) |
 |
Another view of angiofibroma of the nasopharynx, seen from the right nasal passage. |
 |
An involuted papilloma of the nasopharynx. |
 |
A defect created by extensive posterior ethmoidectomy, with extension into the sphenoid sinus. The ostium of the sphenoid sinus is seen beneath the defect. Stellate bands of scar tissue can sometimes produce obstruction leading to a recurrence of chronic sinusitis or mucocele formation. (Selner slide #32) |
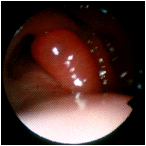 |
This patient has a history of chronic eustachian tube dysfunction causing recurrent middle ear infections. This is the posterior left nasal passage, with the ostium of the left eustachian tube located at 2 o'clock. The lighter tissue at 6 o'clock is the soft palate. An inflammatory polyp is seen protruding from the eustachian tube orifice. (Selner slide #38) |
 |
The left eustachian tube viewed through the right nasal passage. Rosenmuller's fossa is at 9 o'clock and the soft palate, which is not visualized, would be at 6 o'clock. The torus is grossly edematous and has essentially closed the orifice of the eustachian tube. The patient had an associated serous otitis media, however eustachian tube function can not always be predicted by the appearance of the torus. (Selner slide #39) |
In memoriam, John Canty Selner, MD (1936-2006)